Cardiologie interventionnelle - Cas du mois - STCCCV
Complex high risk indicated PCI without mechanical hemodynamic support. What to do ?
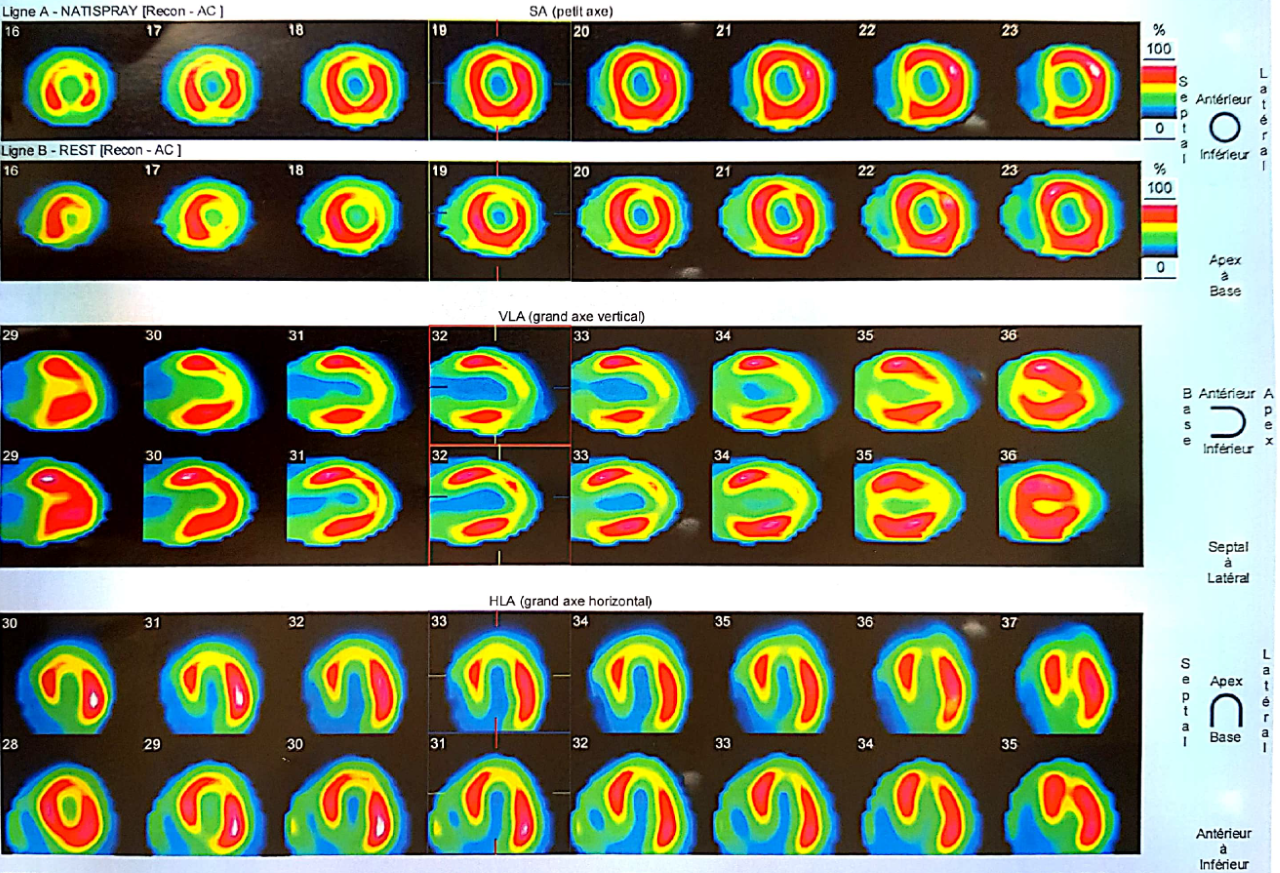
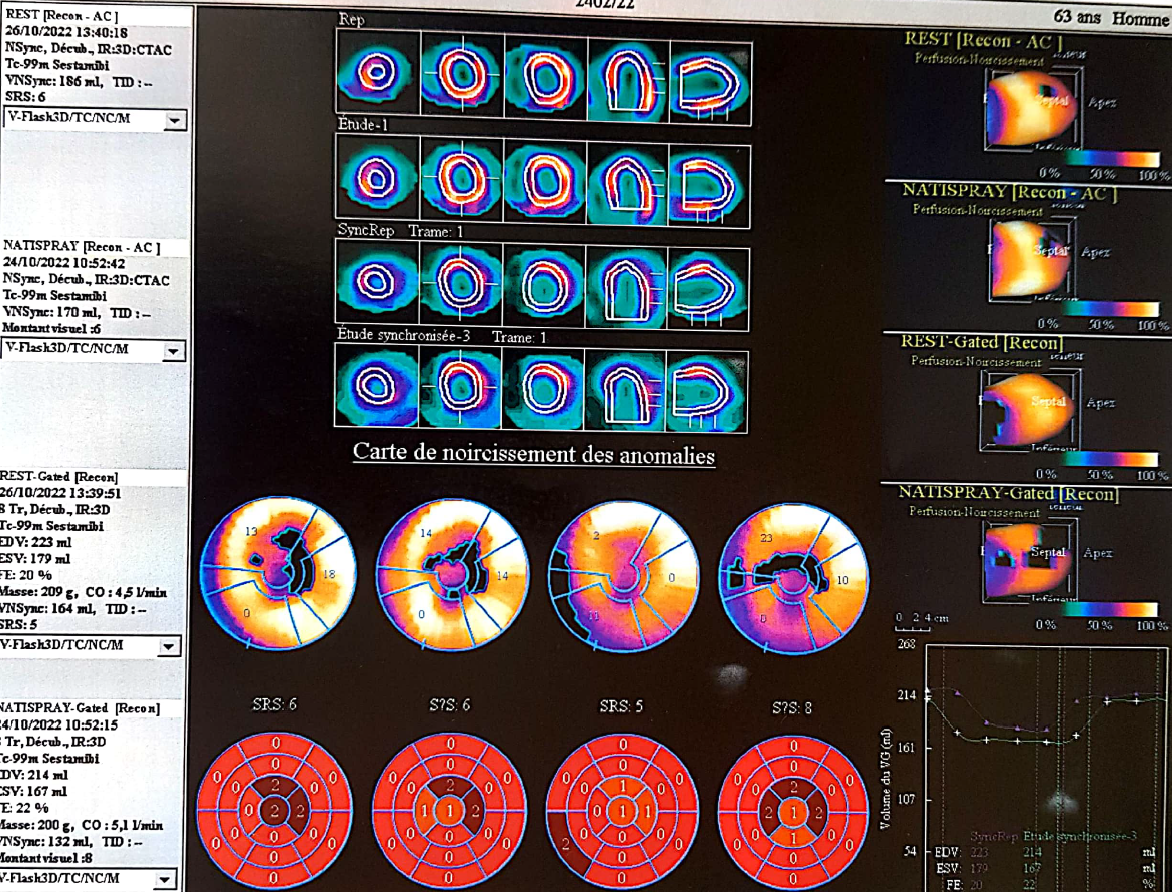
Un homme de 63 ans, ancien fumeur, ayant des antécédents de diabète sucré de type 2, a été transféré des urgences pour un premier épisode d'insuffisance cardiaque aiguë décompensée suite à un NSTEMI. L'échocardiogramme a montré une faible FEVG de 20 % et une fonction VD altérée ( Vidéo 1 ) avec une régurgitation mitrale et tricuspide secondaire importante. ( Vidéo 2 ) Aucun thrombus apical n'a été trouvé. L'entraînement a montré une bonne fonction rénale et aucune anémie. Après les diurétiques de l'anse IV et l'initiation du traitement médical de l'insuffisance cardiaque et du DAPT, le patient est devenu stable, une angiographie coronarienne a été réalisée et a montré une sténose sévère LM, une sténose longue proximale LAD, une sténose sévère OM et RCA CTO ( Vidéo 3). Le PDVG était de 8 mmHg. La viabilité du myocarde à l'exception de l'apex a été confirmée par scintigraphie myocardique. ( Figures 1 et 2 ) Une discussion d'équipe cardiaque a eu lieu…
Les Réponses
What would be the best options to treat this patient?
Réponse et Commentaires
Qu'avons-nous fait ?
Une revascularisation était indiquée mais avec un risque très élevé de complication. Après la discussion de l'équipe cardiaque ; l'option chirurgicale a été refusée principalement en raison d'un dysfonctionnement du VD. Discussion approfondie avec le patient et la famille; sur le pronostic avec toutes les alternatives, leurs risques et avantages a été fait. Le consentement du patient à subir une ICP à haut risque a été obtenu. Quelle serait la stratégie ?
Bien qu'il n'y ait pas d'avantage clair dans l'ECR ; une assistance hémodynamique mécanique était indiquée dans ce cas. En particulier, une pompe à flux axial empêcherait le collapsus hémodynamique pendant la procédure, mais malheureusement, elle n'est pas disponible dans notre contexte.
We assessed first the invasive blood pressure that was 90/60 mmHg. We decided to give IV dobutamine 5µg/Kg/min and noradrenaline 1mg/h to raise the BP to 110/80. Our principal target was LM and proximal LAD lesion but with an RCA occlusion this task was made harder. Beginning with RCA CTO revascularization would reduce the risk of hemodynamic collapse when dilating the LM. After a short antegrade attempt we were not successful so we abandoned this idea decided to tackle left system an take the risk.
We fixed the OM first (Picture 4)
and then LM to LAD with one long DES (Picture 5)
in reverse T stenting fashion. Fortunately all these maneuvers were tolerated by the patient. During the POT with a 5.0 balloon a transient fall of BP resulted in a syncope. After balloon deflation complete recuperation of consciousness and BP of 130/70 was possible without the need to raise vasopressors nor inotropes.
Complete Revascularisation or STOP ?
The patient was stable and the left system PCI was Straightforward 12 min Xray and 80cc of contrast. Leaving the RCA occluded would result in persistent RV dysfunction that would extend hemodynamic compromise and hamper waning of the drugs. Having a wire in the sub-intimal space of the RCA and very good CC 2 collateral from the first septal we decided to attempt shortly a retrograde wiring of the occlusion that was done easily through the stent struts. The retrograde wire found easily the distal true lumen. After a small dilatation of the stent struts the microcatheter followed and we were rapidly set for a reverse cart (Video 6 and 7).
After externalisation; we finally succeeded to have TIMI 3 flow through the RCA after 2 long DES implantation Video 8 and 9.
After 3 months follow-up NYHA improved obviously to stage II and echocardiogram showed a clear increase in LVEF, improvement of RV function and decrease in functional mitral and tricuspid regurgitation (video 10 and 11).
Comments and conclusion
There are still controversies in revascularization of patients with poor LVEF and multivessel disease. STITCH 5 and REVIVED BCIS2 RCTs are negative but our patient was not eligible in both studies.
Studies on MVD and cardiogenic shock are also non applicable in our case.
CHIP patients aren’t rare with population aging and MVD increased prevalence.
Mechanical hemodynamic support; in our case, would have helped preventing hemodynamic collapse and would have made the procedure safer.