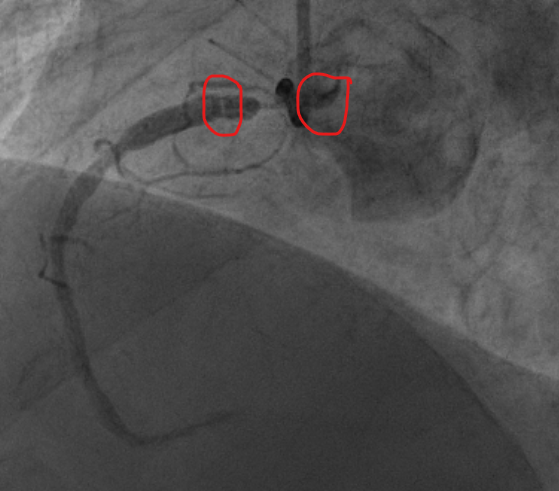
*The most probable origin and course of this RCA is an anterior take-off and small trans-mural course but unfortunately, we didn’t have any imaging modality (pre-angioplasty CT or per-angioplasty IVUS/ OCT) to confirm that and to understand the exact cause of occlusion.
*Even though the support guiding was very poor, I started with antero-grade wire escalation from soft to stiff wire: I used XTR/ Gladius EX/ GAIA 3/Confianza Pro, but I failed because of the “spontaneous intimal dissection” and the lack of support despite the anchoring balloon. I didn’t use a guiding extension because the lesion was very proximal and even the wire couldn’t be maintained in the artery for longtime.
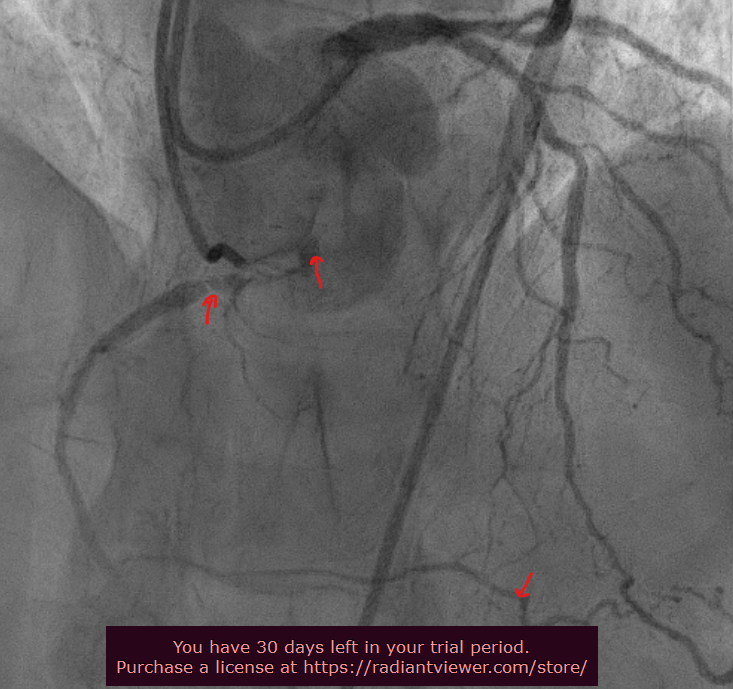
*So I switched to retrograde approach: There wasn’t a promising septal collateral so, I choose to use the epicardial collateral coming from the distal LAD despite its tortuosity. I used a SION Black wire to cross this collateral. The Caravel micro-catheter went smoothly. I did an exchange with a GAIA 3 wire to do the puncture of the distal cap, then I Switched to RG3/300 cm wire. I performed a Homemade snare to retrieve the RG3 wire in the descending aorta. The advancement of the anterograde guiding to the ostium of the RCA (over the trapped retrograde wire) and the TIP IN were unsuccessful. So, the last chance was to inflate a 2.5 mm balloon in the EBU guiding to trap the retrograde wire and then pull all the antero-grade gear to got finally the wire antegradely. I did ballooning and stenting with 2 stents until the ostium of the RCA which was clearly between the left and the right sinus. The final angiogram showed a good result on the RCA and no issue on the collateral and the donor artery.
* There were no peri-procedural complications despite 350 cc of contrast and 5 Gy of radiation.