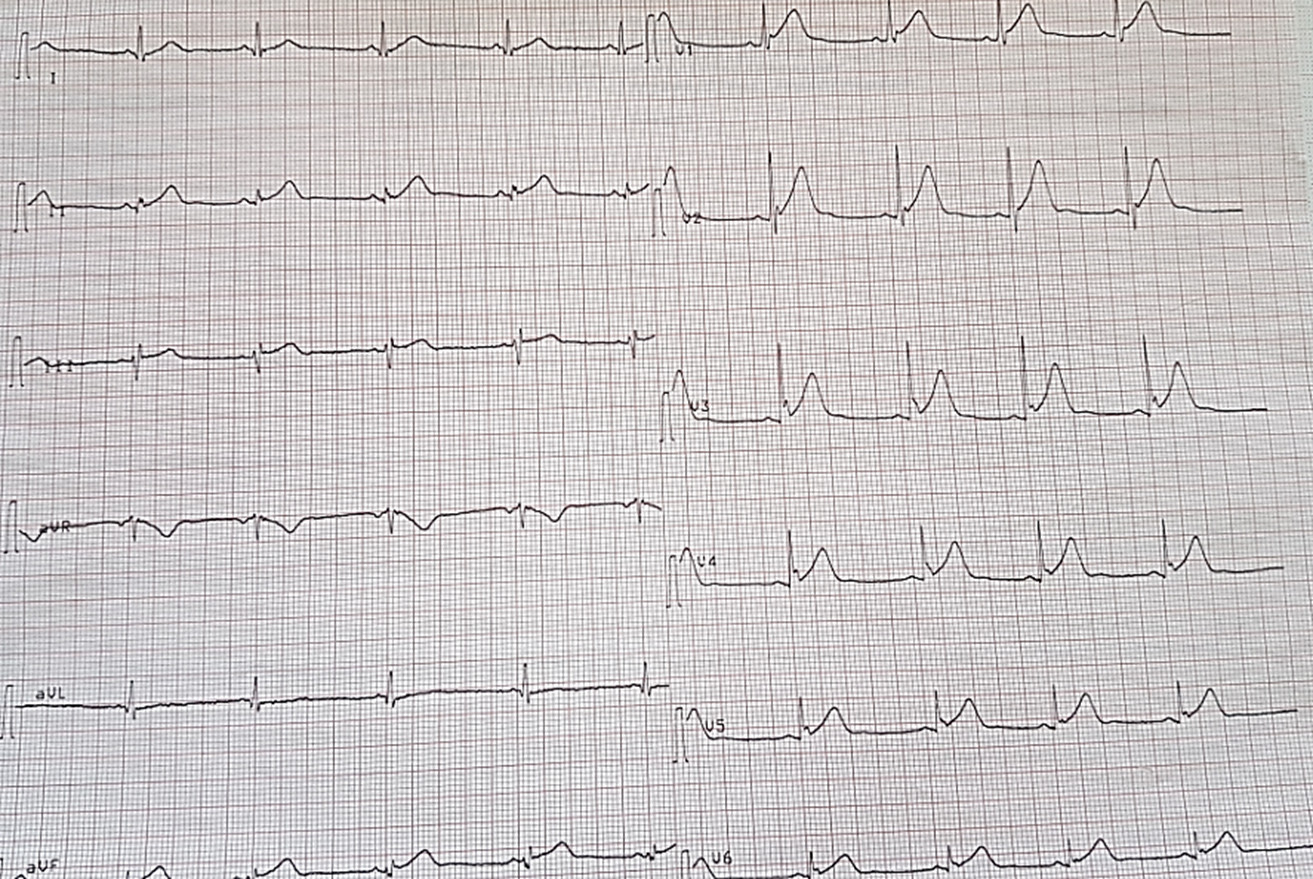
Un homme de 34 ans a été admis dans notre hôpital vu que son défibrillateur implantable (DAI) commençait fréquemment à délivrer des chocs alors que le patient était conscient. Il y a cinq ans, le patient a été implanté d'un DAI simple chambre ( Medtronic) pour un syndrome de repolarisation précoce symptomatique d'une syncope . Son ECG à 12 dérivations au moment de l'implantation du DAI montrait une élévation du point J de 2 mm dans plus de deux dérivations adjacentes avec une encoche sur le complexe QRS terminal (Fig. 1). Il n'y a pas eu de récidive d'arythmie ventriculaire depuis l'implantation.
Le DAI a été programmé avec une zone conditionnelle à plus de 200 battements par minute, une zone de choc à plus de 220 battements par minute. La sensibilité a été programmée à 0,4 mV. L'impédance de la sonde de stimulation était de 589 Ohm et celle de la sonde de choc de 50 Ohm.
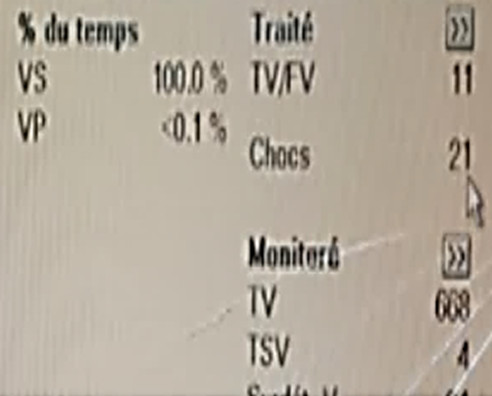
Il a subi un choc de DAI en décembre 2022. L'interrogation du dispositif a révélé une surdétection à haute fréquence sur le canal ventriculaire, interprétée comme une fibrillation ventriculaire par le DAI. Vingt chocs à 34-J ont été délivrés...(Fig 2)
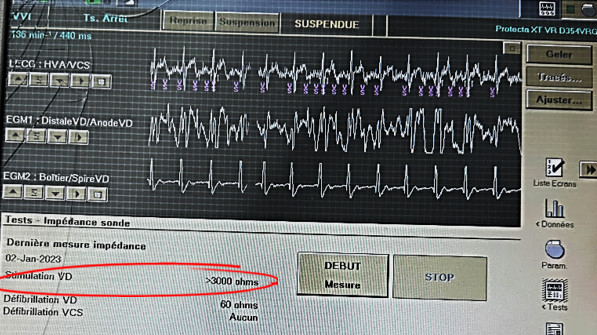
La sonde d'impédance ventriculaire était supérieure à 3 000 ohms. (Fig 3)
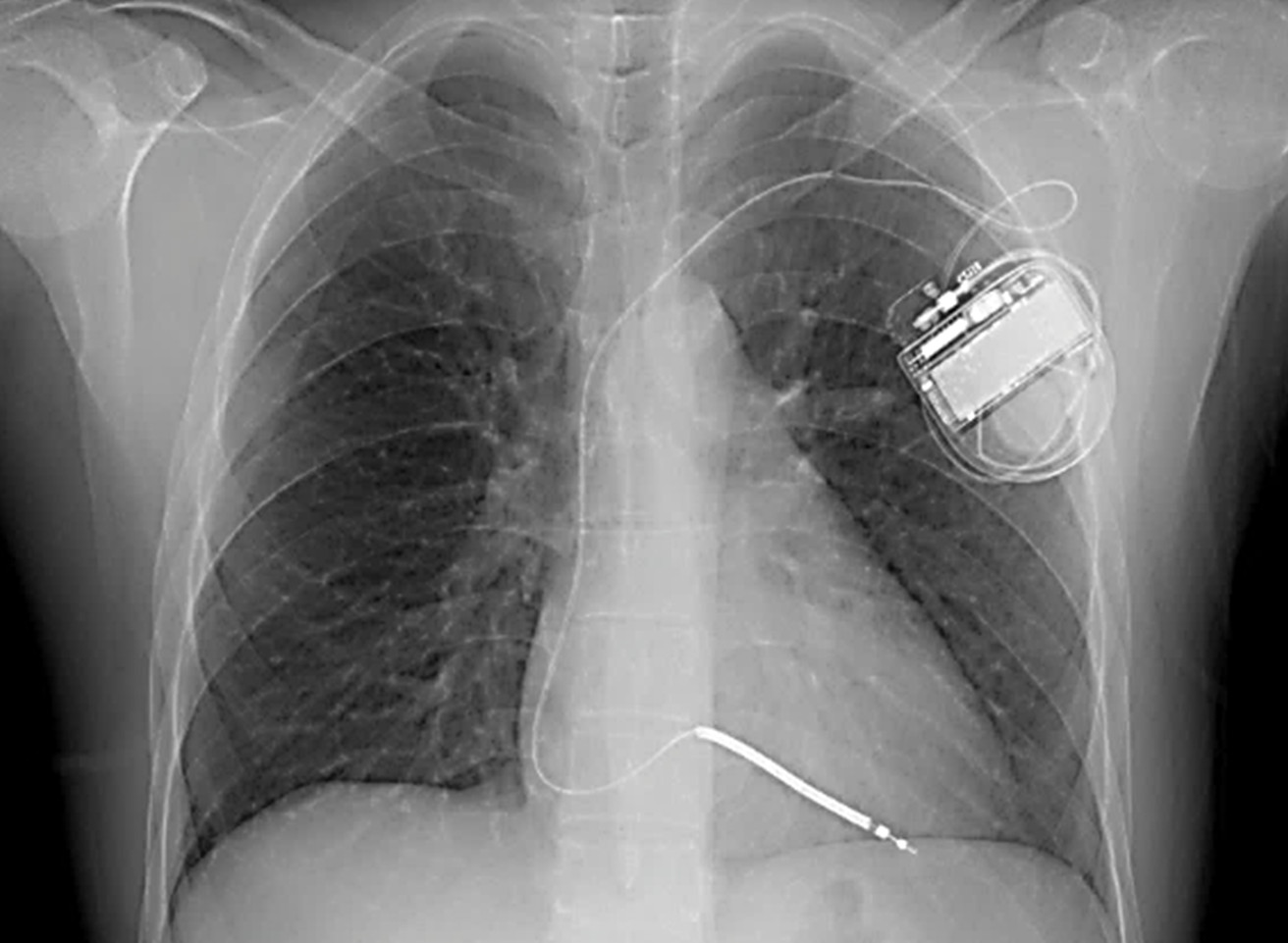
Une radiographie du thorax a été demandée (Fig 4).