*It’s a case of 65 year-old man, diabetic who was symptomatic of angina CCS 2, despite medical treatment, with viable and ischemic inferior wall.
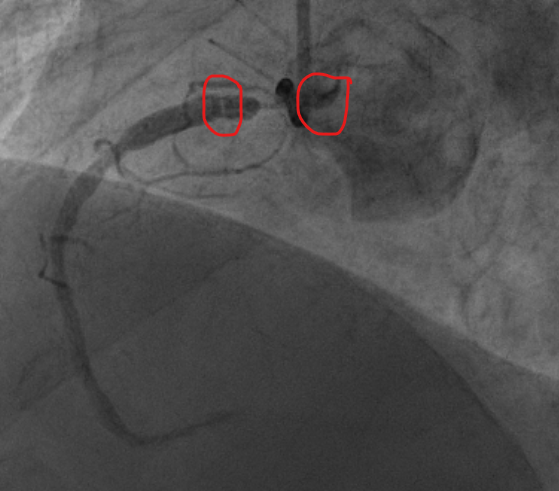
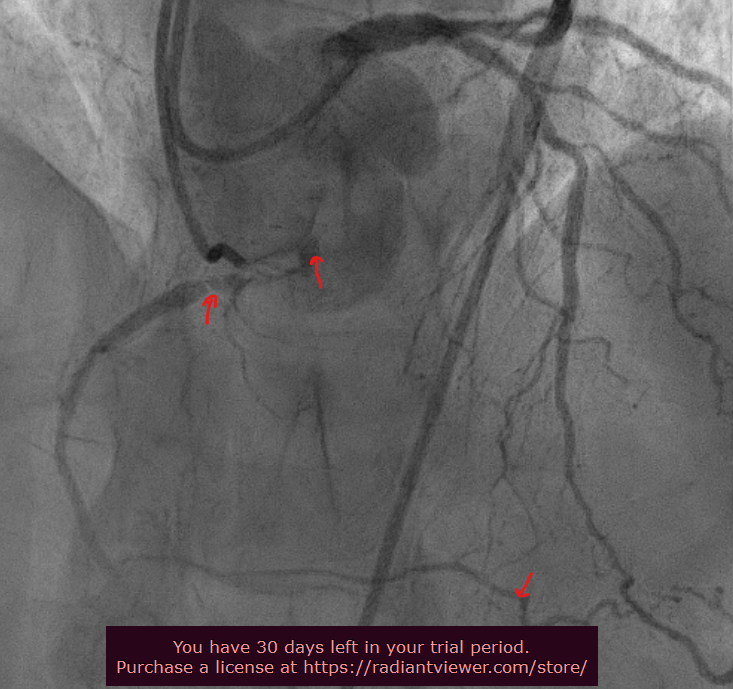
*The selective injection of the RCA was very difficult despite the usage of different types of guiding catheter (JR4, AL0.75, AR1, MP). It showed an abnormal take-off of the ostium and the course of the proximal RCA. We had a very diseased proximal segment followed by a “diaphragm like” lesion. The double injection showed competitive flow in the distality from the distal LAD via a tortuous CC 2 epicardial collateral. There wasn’t a significant disease on the left system.