





A 17-year old man with a history of anxiety presented with several days of intermittent palpitations.
He had recently recovered from an upper respiratory infection. On presentation to the emergency department, he had a heart rate of 180 beats/min and blood pressure of 90/60 mm Hg. His respiratory rate was 25 breaths/min and oxygen saturation: 95% at 30% oxygen concentration. He had no family history of sudden cardiac death and a normal echocardiogram result.
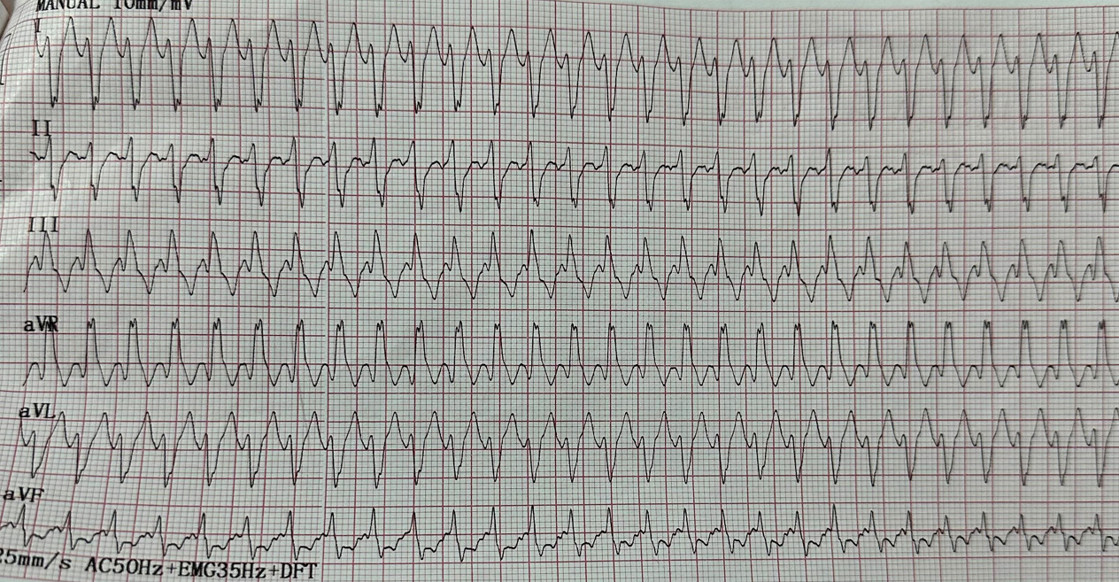
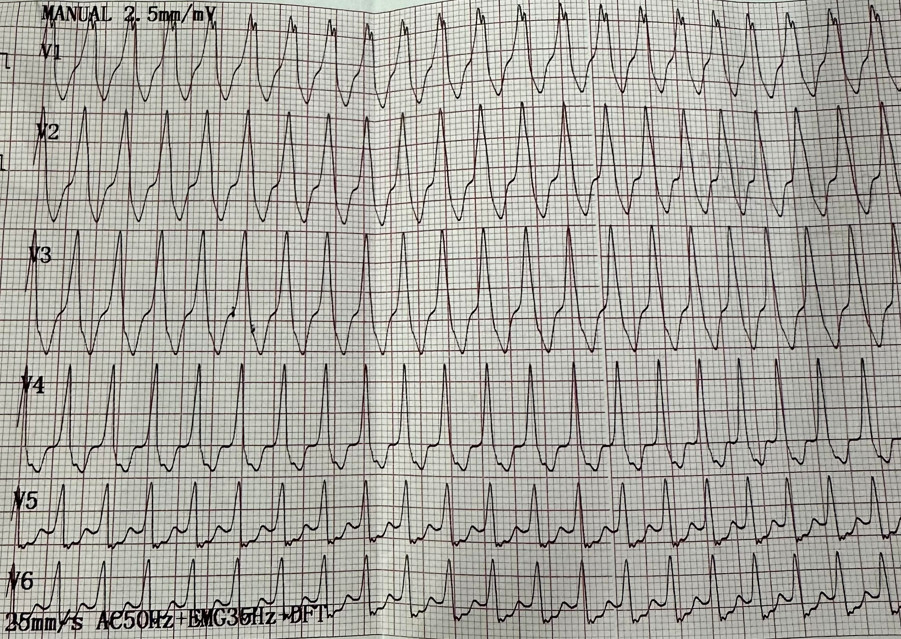
His ECG is shown in Figure 1and 2 with a wide QRS complex tachycardia.
The patient recovers sinus rhythm after IV infusion of 300 of amiodarone. Figure 3
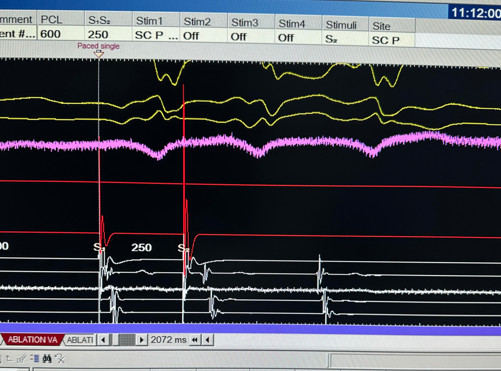
The patient underwent a cardiac electrophysiological study. Multipolar electrode catheters were advanced into the femoral vein and positioned in the right atrium, His-recording region, right ventricular apex, and coronary sinus. Retrograde conduction was existed via the atrioventricular (AV) node. Atrial pacing during tachycardia revealed AV conduction and a ventricular-atrial response. Figure 4

What is the diagnosis of the wide QRS complex tachycardia?