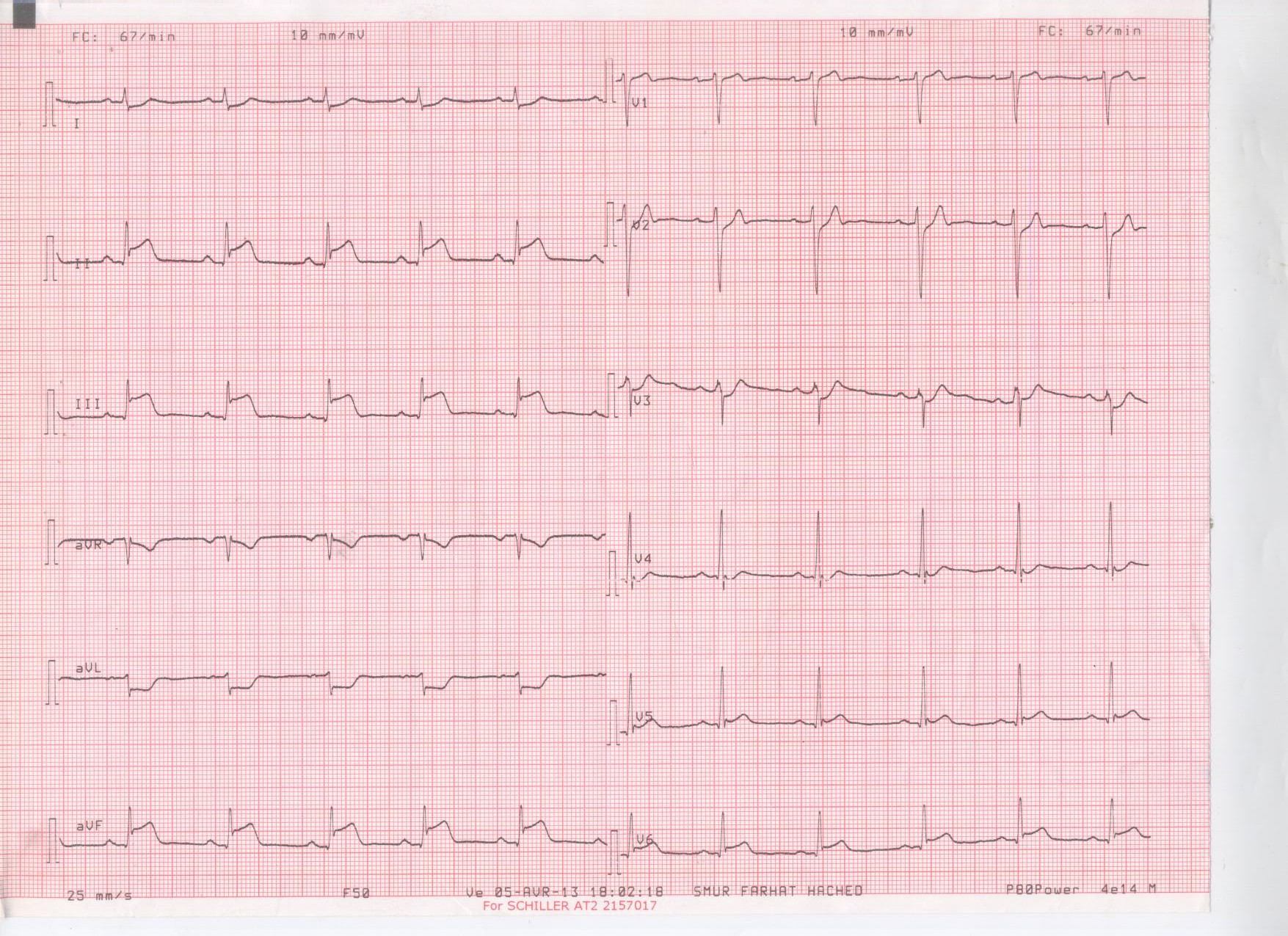
A 28-year-old man presented to the emergency department of a peripheral hospital with acute chest pain that started about 45 minutes ago. The pain was very suggestive: oppressive retro-sternal pain with irradiation to the left forearm. He reported no cardiovascular risk factors except for smoking estimated to 20 cigarettes per day over the past 10 years. The physical examination showed a symmetrical blood pressure of 140/80 mm Hg, a heart rate of 78 bpm, oxygen saturation was 98% spontaneously, cardiac auscultation showed regular heart sounds without murmurs, and there were no signs of heart failure. The ECG showed ST-segment elevation in the inferior leads (II, III, aVF) with ST-segment depression in the anterior leads (Figure 1). Trans-thoracic echocardiography rapidly ruled out pericardial effusion and showed moderate impairment of left ventricular function in relation to hypokinesia of the mid-anterior and the inferior segments.
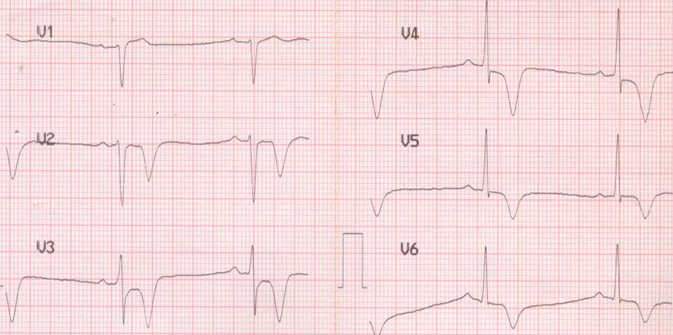
The diagnosis of inferior STEMI was retained and a fibrinolytic treatment was decided as "The door to balloon time" was > 2 hours. On arrival at the tertiary center, the ECG performed 90 minutes after fibrinolysis showed complete regression of ST-segment elevation in the inferior leads with the appearance of negative T waves in the anterior leads (from V2 to V6). Figure 2
Coronary angiogram performed the next day showed a left-dominant coronary circulation with a short and normal left main, a mid narrowing in the mid LAD with normal TIMI flow, the left circumflex as well as the RCA were normal (Figure 3,4).
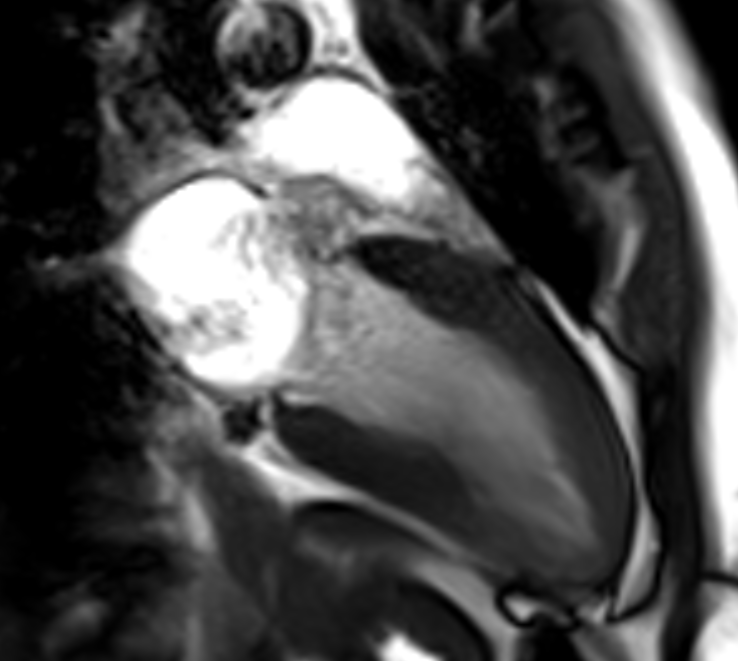
Facing this MINOCA, an MRI was performed which detected an apical wall infarction with severe hypokinesis in the mid and apical segments of the anterior wall associated to T2-weighted high signal due to edema (Figure 5, video 1) .